Situation:
We are third year nursing students in the Nursing Education Program of Saskatchewan on 6300 neurosciences at Royal University Hospital. The purpose of this blog is to present a case study of a client on the ward during our clinical rotation whom we considered to be a complex patient.
We are presenting this case study to further facilitate our learning of caring for a complex patient on a neurology based unit. We also hope that our experience will provide an opportunity for the visitors to this site to gain a similar knowledge base and understanding by accessing our research, plan of care and various linked resources.
Background:
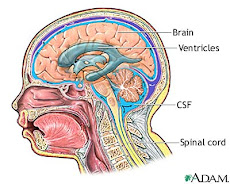
Wilbur Longbottom is an 82 year old male who presented at Saskatoon City Hospital ER on January 30th 2009 with confusion, aphasia and right sided weakness. He was transferred to St. Paul’s Hospital for a head CT which illustrated an intraventricular hemorrhage (IVH) beginning in the left lateral ventricle and expanding to include the third right ventricle and temporal lobe. He also had mild hydrocephalus. He was next transferred to Royal University Hospital (RUH) where an external ventricular drain (EVD) placed to maintain intracranial pressure within normal limits. His blood work demonstrated an increased INR of 4.1 and elevated white blood cells (WBC).
He has a history of atrial fibrillation, gastric ulcers, hypothyroidism, and hypertension. He was on warfarin at the time of admission for treatment of atrial fibrillation.
He remained in the RUH intensive care unit for 5 days. On February 4th, he was extubated but was unable to maintain a patent airway and a #6 cuffed Shiley tracheotomy was placed. On February 5th he was admitted to the observation unit on 6300 with a fluctuating Glasgow Coma Scale (GCS) of between 9 and 11. His GCS has remained fluctuating between 9 & 11 throughout the five days he had been in observation. He had a 3 lumen Foley draining frank hematuria as a result of traumatic insertion and wears benefits for bowel incontinence. He was independent of all ADL’s before this hospitalization. His increased WBC count was also of concern and he was under investigation for query meningitis.
Assessments:
Caring for complex patients is multifaceted and nurses must be competent in general head to toe assessments with the ability to focus each assessment according to the specific needs of the patient. For this patient our focus would be on the neurological system paying specific attention to the Glasgow Coma Scale, LOC, behavioural or physical changes that may indicate increased ICP, and the muscular strength of the patient. Monitoring for signs of infection is also essential as he has an EVD which provides a direct entry into the brain and already has an elevated WBC count. Other key skills for nursing this client include reading ECGs, competent medication management, interpreting blood work and monitoring for signs of clots as he has atrial fibrillation but is no longer on warfarin. We would also monitor for bleeding as he has already experienced a cerebral bleed and has gross hematuria.
Recommendations:
We recommend that other students access the links on this page to gain a better understanding of the diagnostics and procedures involved with Wilbur Longbottom. Many of these procedures are relevant to numerous patients with neurological injuries and disorders and therefore the knowledge from this case can be transferred to other situations, adding to our knowledge base as health care providers.
Complexity
In the article, “Case and Care Complexity In the Medically Ill”, defines complexity as multi-morbidity, more specifically as a “complex adaptive system that consists of individual agents with the freedom to act in ways that are not always totally predictable, and those actions are interconnected so that one agents actions changes the context for other agents” (Jonge, Huyse, & Stiefel, 2006, p. 679). Complexity arises when several systems or disease processes interact, sometimes resulting in overlapping symptomology, referred to as case complexity. This article also includes psychiatric co-morbidities, such as frailty and depression, which are often overlooked in the complexity system (Jonge et al., 2006). This model of complexity derives its focus from medical conditions with the interaction of multiple systems along with considerations of psychosocial condition of the client.
Complexity science as defined by Wilson , Halt & Greenhalgh (2001) suggests that illness results from complex and unique interactions in both the physical and psychosocial systems; any small differentiation in any one system will cause an imbalance throughout the remaining systems. Interaction between the systems is the cause of disease complexity, not just a single components malfunction. It also suggests that we as care providers have to take a more holistic approach in our treatment towards our clients. The holistic approach is looking at the relationships between interacting body systems, the behaviour, the environment and the beliefs of the patient which are dynamic and fluid.
Comparing the perception of complexity between these two articles, similarities are apparent at first, yet differences arise with further analysis. Comparing similarities, each focuses on systems interactions as the cause of complexity within the patient. Wilson et al (2001) states, “Human beings can be viewed as composed of and operating within multiple interacting and self adjusting systems (including biochemical, cellular, physiological, psychological, and social systems)” (p. 685). Jonge et al (2006) have a similar perception as they also focus on the interactions of systems which then in turn results in patient complexity.
Differences with these two definitions of complexity stem from the specific considerations of systems interactions. Jonge et al (2006) incorporates main body systems as the interacting determinants for complexity, more specifically psychological and somatic medical issues. One specific example used is the relationship between metabolic syndrome, depression, and cardiovascular disease which focused on the physical ramifications of these interacting diagnoses. Wilson et al (2001), however has a broader definition and scope for looking at complexity. Although the risk factors and symptoms play a role, a wider perspective including all aspects of the patients past experiences and adaptive responses to their new environment are incorporated (p. 685). Wilson et al (2001) perception is also more consistent with the holistic goals of providing nursing care. As future nurses, identifying the importance to consider the patient in a holistic view will aid in providing improved quality of nursing care as compared to the specific focus on only patient medical diagnosis.
Wilbur Longbottom is an eighty two year old male with a history of hypothyroidism, atrial fibrillation, hypertension, gastric ulcer and “kidney problems”. He has had a cholecystectomy and “fluid in lungs“ in early January, as well as hearing problems. Patient was diagnosed by CT as having an intraventricular hemorrhage, possible cause being an increased INR of 4.1. An EVD was placed to control his intracrainial pressure, and he was then placed in ICU. A tracheostomy was also placed due to his inability to maintain his airway; hematuria is also present due to a traumatic catheter insertion. The patient was then transferred to neurology 6300 after six days in ICU, and has been in observation since the transfer due to a fluctuating GCS. There is also suspicion of query meningitis not yet diagnosed.
This patient matches the presented standard of complexity with his current medical state which include all body systems, interactions among these and overlapping symptomology. In the central nervous system he has intraventrical hemorrhage and problems with fluctuating GCS. In the cardiovascular system his history of atrial fibrillation has led him to be placed on Warfarin; which has caused his increased INR levels, thus IVH, he also has a history of hypertension. He was unable to maintain a patent airway in hospital and because of this his respiratiory system is also affected, he has a tracheostomy, copious amounts of creamy yellow secretions, fluid to bases of lungs, and has been placed on aspiration precautions. This patient has history of gastric ulcers which are being treated with prescription Ranitidne; which is known to interfere with warfarin clearance. Mr Longbottom has also pulled out his NG tube and is awaiting a modified barium swallow test, but until that test he is NPO. In genitourinary he has a three way catheter inserted and has had hematuria related to a traumatic insertion, and is currently using benefits. Mr Longbottom is currently on numerous diuretics for his HTN, this coupled with his history of “kidney problems” puts him at greater risk of kidney failure. His integumentary has been impaired by the surgery, and he has a large incision to his head with an EVD, this device has greatly reduced Mr. Longbottom's mobility which may possibly lead to a breakdown of his skin. The patient has a history of hypothyroidism and is on levothyroxine for this, he is also currently on Humulin R as per standard aftercare of neurosurgery patients. This is because the body has an altered stress response and may not be producing enough insulin naturally.
Sometimes overlooked but equally important are psychological issues the patient is facing (Jonge et al, 2001). This patient is experiencing impaired speech and thus unable to verbalize his needs. He is experiencing frustration due to this as he loved to talk previous to hospitilazation. According to Mr. Longbottom's wife, prior to this admission he was independent and this loss of independence coupled with not being able to do normal ADL's may lead to further frustration for both the patient and his family.
References
Jonge, P., Huyse, F.J., Stiefel, F.C. (2006). Case and care complexity in the medically ill.
The Medical Clinics of North America. 90(1), 679-692.
Wilson, T., Holt, T., Greenhalgh, T. (2001). Complexity science: Complexity and
clinical care.323; 685-688. Retrieved February 23, 2009 from bmj.com.
Complexity science as defined by Wilson , Halt & Greenhalgh (2001) suggests that illness results from complex and unique interactions in both the physical and psychosocial systems; any small differentiation in any one system will cause an imbalance throughout the remaining systems. Interaction between the systems is the cause of disease complexity, not just a single components malfunction. It also suggests that we as care providers have to take a more holistic approach in our treatment towards our clients. The holistic approach is looking at the relationships between interacting body systems, the behaviour, the environment and the beliefs of the patient which are dynamic and fluid.
Comparing the perception of complexity between these two articles, similarities are apparent at first, yet differences arise with further analysis. Comparing similarities, each focuses on systems interactions as the cause of complexity within the patient. Wilson et al (2001) states, “Human beings can be viewed as composed of and operating within multiple interacting and self adjusting systems (including biochemical, cellular, physiological, psychological, and social systems)” (p. 685). Jonge et al (2006) have a similar perception as they also focus on the interactions of systems which then in turn results in patient complexity.
Differences with these two definitions of complexity stem from the specific considerations of systems interactions. Jonge et al (2006) incorporates main body systems as the interacting determinants for complexity, more specifically psychological and somatic medical issues. One specific example used is the relationship between metabolic syndrome, depression, and cardiovascular disease which focused on the physical ramifications of these interacting diagnoses. Wilson et al (2001), however has a broader definition and scope for looking at complexity. Although the risk factors and symptoms play a role, a wider perspective including all aspects of the patients past experiences and adaptive responses to their new environment are incorporated (p. 685). Wilson et al (2001) perception is also more consistent with the holistic goals of providing nursing care. As future nurses, identifying the importance to consider the patient in a holistic view will aid in providing improved quality of nursing care as compared to the specific focus on only patient medical diagnosis.
Wilbur Longbottom is an eighty two year old male with a history of hypothyroidism, atrial fibrillation, hypertension, gastric ulcer and “kidney problems”. He has had a cholecystectomy and “fluid in lungs“ in early January, as well as hearing problems. Patient was diagnosed by CT as having an intraventricular hemorrhage, possible cause being an increased INR of 4.1. An EVD was placed to control his intracrainial pressure, and he was then placed in ICU. A tracheostomy was also placed due to his inability to maintain his airway; hematuria is also present due to a traumatic catheter insertion. The patient was then transferred to neurology 6300 after six days in ICU, and has been in observation since the transfer due to a fluctuating GCS. There is also suspicion of query meningitis not yet diagnosed.
This patient matches the presented standard of complexity with his current medical state which include all body systems, interactions among these and overlapping symptomology. In the central nervous system he has intraventrical hemorrhage and problems with fluctuating GCS. In the cardiovascular system his history of atrial fibrillation has led him to be placed on Warfarin; which has caused his increased INR levels, thus IVH, he also has a history of hypertension. He was unable to maintain a patent airway in hospital and because of this his respiratiory system is also affected, he has a tracheostomy, copious amounts of creamy yellow secretions, fluid to bases of lungs, and has been placed on aspiration precautions. This patient has history of gastric ulcers which are being treated with prescription Ranitidne; which is known to interfere with warfarin clearance. Mr Longbottom has also pulled out his NG tube and is awaiting a modified barium swallow test, but until that test he is NPO. In genitourinary he has a three way catheter inserted and has had hematuria related to a traumatic insertion, and is currently using benefits. Mr Longbottom is currently on numerous diuretics for his HTN, this coupled with his history of “kidney problems” puts him at greater risk of kidney failure. His integumentary has been impaired by the surgery, and he has a large incision to his head with an EVD, this device has greatly reduced Mr. Longbottom's mobility which may possibly lead to a breakdown of his skin. The patient has a history of hypothyroidism and is on levothyroxine for this, he is also currently on Humulin R as per standard aftercare of neurosurgery patients. This is because the body has an altered stress response and may not be producing enough insulin naturally.
Sometimes overlooked but equally important are psychological issues the patient is facing (Jonge et al, 2001). This patient is experiencing impaired speech and thus unable to verbalize his needs. He is experiencing frustration due to this as he loved to talk previous to hospitilazation. According to Mr. Longbottom's wife, prior to this admission he was independent and this loss of independence coupled with not being able to do normal ADL's may lead to further frustration for both the patient and his family.
References
Jonge, P., Huyse, F.J., Stiefel, F.C. (2006). Case and care complexity in the medically ill.
The Medical Clinics of North America. 90(1), 679-692.
Wilson, T., Holt, T., Greenhalgh, T. (2001). Complexity science: Complexity and
clinical care.323; 685-688. Retrieved February 23, 2009 from bmj.com.
Prep Guide and Medications
Students: Steph, April, Serena, Joelle, Traci and Jason
Date: Feb. 11, 2009
Patient: Wilfred Longbottom
Age: 82
Residence: Saskatoon
Admission Date: Jan. 30, 2009
Admitting Diagnosis: Intraventricular hemmorhage r/t increased INR (4.1)
Diet:
Past Medical History
Date: Feb. 11, 2009
Patient: Wilfred Longbottom
Age: 82
Residence: Saskatoon
Admission Date: Jan. 30, 2009
Admitting Diagnosis: Intraventricular hemmorhage r/t increased INR (4.1)
Diet:
- NPO Promote @ 15cc/ hr (increase 10cc/hr until at goal of 85 cc/hr) This was discontinued as the patient pulled out his duotube and Feb 11th was given full thickened fluids with supplements
Past Medical History
- Cholecystectomy
- Gastric ulcer
- Hypothyroidism
- Kidney problems
- Atrial fibrillation
- Increased INR
- HOH
- Fluid in lungs early January
- Hypertension
- Presentation to Hospital
Jan 30th – confusion while driving, decreased motor skills, decreased speak, son brought him to SCH
Social History
- Lives with wife in house (bungalow, 1 level), no use of community resources for ADLs.
Psychological History - has son in city
- occasional social drinker
- Zero smoking or drugs
- has son in the city
- Wife to visit, is ++ worried that Wilbur will not recover
- Close family ties
- Retired CN engineer
- Daily visitors (wife, son and neice)
Psychological History
- Attempting to pull out NG/EVD
- Restrained
- Loves to talk according to wife
Course in Hospital
Admission ward:
- Emerg SCH
Ward Transfers:
- SPH for CT then to RUH for neurosurg to ICU then Feb 5th to 6300
Results of Important Diagnostics Tests:
Jan 30th
- CT: blood in L lateral ventricle expanding into 3rd R ventricle and temporal
Feb 6th:
- CXR fluid to bases of lungs
Feb10th
- WBC 13.46 (H); neutrophil 10.58 (H); lymphocyte 1.3 (L); monocyte 1.3 (H)
K 3.1 (L), Cl 93 (L) CO2(total) 36 (H) urea 8.3 (H) - CSF (appearance cloudy red fluid)
- CSF differential neutrophil 66%, lymphocytes 6% macrophages 28%
- micro: ventricular fluid moderate polymorphnuclear WBC; sputum abundant polymorphnuclear WBC, moderate squamous epithelial cells, few gram pos bacilli
general 1.B increase sensitive CRP 30.2 (H) (systemic inflammation)
prealbumin 148 (L)
Surgical Events:
- Placement of EVD January 30
- Tracheotomy put in February 4th
Response to treatment:
- GCS: Ranging from 9-11/15
- R paraesis
- edema to extremities
- creamy yellow secretions in tracheotomy
Complications:
- Query ileius and meningitis
- Risk for aspiration pneumonia
- Hematuria
Adverse events:
- Seizures (partial L arm and face)
Discharge planning:
- Working toward maintaining patient stablility and begin rehabilitation. Patient likely unable to return home, consult with CPASS and discuss with family.
Medical Plan of Care:
Focus of Care: Diagnositic and Rahabilitative
- Consults: PT/OT, Urology, General Surg, SLP, NSS, Infectious diseases
- Tests: CBC, lytes 6, TENS bloodwork. daily coags, EEG, ECG, renal U/S CXR, CT, sputum c&s, U/A CSF, MRSA swab (Monitor Diagnostics)
- Medication management
- Pain management
- Nutritional status
Nursing Plan of Care:
Nursing Focus: Rehabilitative and Supportive
- Neurological focus
- Medication management
- Monitor diagnostics
- Pain management
- Supportive care
- Patient and family teaching
- Identify family supports (Possible SW consult)
- Monitor fluid balance
Degree of Stability:
- Stable - Vital Signs: 37.2-66-16 125/70 99% trach hood 35% O2 humidified
Medication Names, Anticipated Effects and Common Side Effects:
levothyroxine 0.1 mg via PO OD 0800
- Class: thyroid hormone
- Receiving for hypothyroidism prior to hospitalization which will maintain secretion of T3 hormone.
- Nervousness insomnia, tremor, tachycardia, palpitations, angina, dysrrhythmias, nausea, diarrhea, cramps, weight loss, fever.
amlodipine besylate (Norvasc) 15 mg PO OD 0800
- Class: antianginal, antihypertensive, calcium channel blocker.
- Treatment of patient hypertension by producing relaxation of vascular smooth muscle and dilating coronary vascular arteries also increasing myocardial oxygen delivery.
- Edema, headache, dysrrhythmias, anxiety, nausea, vomiting, diarrhea, nocturia, flushing, weight gain.
atenolol 100 mg PO/NG OD 0800
- Class: beta blocker, antihypertensive, antianginal
- Maintenance of blood pressure and atrial fibrillation by producing negative inotropic and chronotropic effect.
- fatigue, dizziness, hypotension, mental changes, cold extremities, postural hypotension, second and third degree heard block, nausea, diarrhea.
Insulin Humulin R 100 units/ml SC by sliding scale 1000
- Class: antidiabetic, pancreatic hormone
- Control blood glucose levels d/t clients inability to maintain own in relation to altered health status and stress.
- Hypoglycemia, dry mouth, lipodystrophy, blurred vision, flushing, rash, rebound hyperglycemia.
- Class: antihypertensive, ACE inhibitor
Maintenance of blood pressure by inhibiting development of potent vasoconstrictor angiotensin 2. - Hypotension, hyperkalemia, insomnia, dizziness, tinnitus, dry cough.
- Class: H2 histamine receptor antagonist.
- Treatment of gastric ulcer by inhibiting histamine at H2 receptor sites thus decreasing gastric acid secretion.
- headache, confusion, tachycardia, bradycardia, constipation, abdominal pain, nausea, vomiting, blurry vision.
**known to increase the toxicity of anticoagulants, client is on Warfarin.
- Class: Loop diuretic
- Maintenance of blood pressure through inhibiting reabsorption of NA and Cl thus decreasing vascular fluid volume and excreting it through the kidneys.
- polyuria, hypocalemia, hyponatremia, hypokalemia, hypomagnesemia, hyperuricemia, hyperglycemia, nausea, rash, pruritus, hypochloremia
- Class: thiazide diuretic, antihypertensive
- Maintenance of blood pressure by increasing excretion of water, Na, K, and Cl. This decreases vascular fluid volume by excreting it through the kidneys.
- orthostatic hypotension, polyuria, hypokalemia, dizziness, hyponatremia, hypochloremia, nausea, vomiting, weakness, anorexia, hyperglycemia.
- Class: anticonvulsant, antidysrrhythmia
- Seizure prevention used as a prophylactic after neurosurgery. Works by altering ion transport at the motor cortex to inhibit the spread of seizure activity.
- ataxia, decreased coordination, mental confusion, slurred speech, diplopia, nystagmus, hyperplasia, N&V.
- Class: antihypertensive, direct acting peripheral vasodilator
- Maintenance of blood pressure through decreasing vascular resistance through vasodilatation.
- headache, angina pectoris, palpitations, tachycardia, N&V diarrhea, anorexia, lupus-like syndrome, headache, tremors, dizziness, anxiety.
- Class: anti-infective
- Prophylaxis after surgical procedure to prevent development of infection. Patient at particular risk d/t EVD. Inhibits bacterial cell wall synthesis causing cell death.
Query pneumonia - fever, pain, hypotension, ototoxicity, tinnitus, leukopenia, neutropenia, superinfection, increase BUN, Creatinine and albumin.
- Class: Broad-spectrum antibiotic, 3rd generation cephalosporin
- Prophylaxis after surgical procedure to prevent development of infection. Patient at particular risk d/t EVD. Causes osmotic instability leading to cell death.
Query pneumonia - phlebitis, thrombophlebitis, macropapular and erythematous rashes, urticaria, pain, sterile abcessess, temperature elevation,
clonidine 0.1 mg PO Q1H PRN for SBP> 150
- Class: antihypertensive
- Alleviate hypertension by decreasing BP, pulse rate, and cardiac output.
- drowsiness, dizziness, sedation, constipation, dry mouth, pruritis, fatigue, orthostatic hypotension, palpitations, CHF, nausea, vomiting, rash, depression.
acetaminophen/codeine 325-30 1-2 tab PO Q4H ORN
- Class: opiate analgesic, antitussive, antipyretic.
- Treatment of moderate pain by depressing pain impulse transmission and improving client comfort.
- constipation, headache, drowsiness, sedation, seizures, circulatory collapse, bradycardia, lethargy, nausea, vomiting, anorexia, urinary retention, flushing.
- Class: opioid analgesic
- Treatment of moderate to severe pain by depressing pain impulse transmission and improving client comfort.
- constipation N&V, euphoria, clouded sensorium, bradycardia, shock, cardiac arrest, respiratory depression, respiratory arrest, apnea, palpitations, urinary retention, constipation.
dimenhydrinate 25-50 mg IV/PO Q4H PRN
- Class: antiemetic, antihistamine, anticholinergic
- Treatment of motion sickness, nausea, vomiting and vertigo. Effects result in decreased vestibular stimulation and blockade of chemoreceptor trigger zone.
- Drowsiness, hypotension, dry mouth, constipation, nasal congestion, restlessness, insomnia, hypertension, palpitations.
- Class: nonopioid analgesic, antipyretic
- Treatment of mild by blocking pain impulses peripherally. Treatment of fever through inhibition of prostaglandins in CNS.
- Hepatotoxicity, hepatic seizures, renal failure, anemia, stimulation, drowsiness, nausea, vomiting, abdominal pain, rash.
- Class: laxative, saline
- Treatment of constipation by increasing peristalsis and water retention.
- Dysrhythmias, cardiac arrest, hypotension, nausea, cramps, diarrhea, electrolyte and fluid imbalance, widening QRS complex.
- Class: laxative, stimulant
- Short-term treatment of constipation by acting directly on the intestine and increasing motor activity.
- Muscle weakness, nausea, vomiting, anorexia, cramps, rectal bleeding, tetany, hypokalemia, electrolyte and fluid imbalance.
- Class: laxative-stimulant
- Treatment of acute constipation by stimulating peristalsis and softening feces by increasing water and electrolytes in the large intestine.
- Nausea, vomiting, anorexia, cramps, diarrhea, flatulence, hypocalcemia, tetany.
Docusate sodium syrup 100 mg/25 mL 100-200 mg PO BID PRN
- Class: laxative, emollient, stool softener.
- Treatment of constipation by increasing water, fat penetration in intestine thus allowing for easier passage of stool.
- Bitter taste, throat irritation, nausea, anorexia, cramps, diarrhea, rash.
Care Plan, Head to Toe Assessment and Neuro Vitals
Nursing Diagnoses:
1. Compromised airway r/t altered LOC evidenced by fluctuating GCS levels within the past 24 hours.
Evidence:
- Fluctuating GCS of 9-11
- Tracheotomy
- Occasional Restraints to prevent pulling of IV
- Confusion
- Bedrest
- Thick creamy secretions
- Diet: Full thickened fluids
- Patient risk for aspiration.
Interventions
- Apply suction prn to maintain clear airway when secretions are present.
- Administer analgesics to maintain patient comfort (shallow breathing can be induced by pain d/t discomfort)
- Encourage deep breathing and coughing
- Hyperoxygenate before and after tracheal suction
- Maintain patient hydration and encourage fluids to liquefy thick secretions
- Assess patient oxygen saturation and respiratory rate, assess present oxygen therapy devices.
- Auscultate breath sounds and assess air movement to monitor and record status.
- Observe for signs of respiratory distress (increased rate, restlessness/anxiety, use of accessory muscles for breathing)
- Observe for improvement in symptoms
- Contact respiratory therapy to assess the patient’s respiratory situation
- Monitor the blood gas values
- Educate the patient and family on why he has a tracheotomy, what your monitoring for and answer any questions they might have
2. Altered cerebral tissue perfusion r/t IVH and EVD placement.
Evidence:
- EVD-draining cloudy red CSF
- Hydrocephalus
- Increased Intracranial pressure
Fluctuating GCS - Aphasia
- Decreased ADL’s
- Confusion
- Bedrest
- Right sided weakness
- Atrial Fibrillation
- Discontinued anticoagulant therapy
- Bowel and Bladder Incontinence
Interventions
- Neuro vitals q2h
- Assess for purposeful and non-purposeful motor responses, compare right and left sides.
- Decrease extraneous stimuli/provide comfort measures (ex. Quiet environment and rest) to reduce CNS stimulation.
- Monitor/document changes in LOC and indications of increased ICP (pupils, headache, numbness/tingling).
- Monitor vital signs
- Provide safety measures to prevent injury (side rails, assess restraints frequently)
- Assess the patient’s pain level on a scale of 0-10, administer analgesics prn
- Educate the patient and family on IVD’s & EVD’s, inform them what you are monitoring for and answer any questions they might have
3. Tissue Injury r/t traumatic catheter insertion evidenced by gross hematuria.
Evidence:
- Gross hematuria
- 3 way Foley Catheter inserted
- Discontinued anticoagulant therapy
- Previously high INR
- Cerebral hemorrhage
Interventions
- Investigate urology consult.
- Assess I&O and characteristics of output (amount of hematuria, presence of clots), identify if hematuria has decreased or increased. Document findings.
- Assess signs of bleeding in other areas (nosebleeds, signs of increased ICP, bruising)
- Administer analgesic medication to improve client comfort and relieve pain.
- Assess CBC values for evidence of increased bleeding (decreased RBC, decreased Hemoglobin etc)
- Monitor INR and PTT closely
- Assess skin color and cap refill.
Assess Vitals signs q4h (note BP and HR) - Provide safety measures to prevent injury (side rails, check restraints)
- Educate the patient and family on why blood is in his urine, what you’re monitoring for and answer any questions they might have
Schedule:
Patient Name: Wilfred Longbottom Age: 82 years old Room and Bed #: Obs 2 Bed 3
0800
- Meds (1,2,3), VS (1,2,3), Neuro vitals (1,2)
- Initial Assessment (complete head to toe) (1,2,3), Assess pain-give pain meds prn (1,2,3)
- Check equipment including oxygen therapy devices and side rails (1,2,3)
- Check IV NS @ 120ml/h
- Review I&O sheet from evening shift (3)
- Assess the characteristics of the output (3)
0900
- Encourage DB & C (1)
- Assist with breakfast (1)
- Basin Bath
- Check IV NS @120 ml/h
1000
- Meds (1,2,3)
- Interpret blood gases and take necessary action (1)
- Read lab value & take necessary action (1,2,3)
- Chem Strip
- Check IV NS@120ml/hr
- My break
1100
- Charting (1,2,3)
- Patient and family teaching (2)
- Check IV NS@120ml/hr
1200
- Meds
- VS (1,2,3), Neuro Vitals (1,2)
- Assess pain level (1,2,3)
- Assist with lunch(1)
- Check IV NS@120ml/hr
1300
- Check IV NS@120ml/hr
- My Lunch
1400
- Empty Catheter, record I&O & assess output (3)
- Chem Strip
- Check IV NS@120ml/hr
- Allow the patient a quiet environment to rest (2)
1500
- Check IV NS@120ml/hr
- Patient & family teaching (1,3)
1600
- Vital Signs (1,2,3)
- Neuro Signs (1,2)
- Check IV NS@120ml/hr
1700
- Meds (1,2,3)
- Check IV NS@120ml/hr
- Assist with supper (1)
- My break
1800
- Review charting (1,2,3)
- Chem Strip
- Check IV NS@120ml/hr
- Empty catheter, record I&O & assess output(3)
1900
- Check IV NS@120ml/hr
- Report off
- Report
*Apply suction prn (1)
Head-To-Toe Assessment
Nursing Diagnosis
1. Compromised airway r/t altered LOC evidenced by fluctuating GCS levels within the past 24 hours.
2. Altered cerebral tissue perfusion r/t IVH and EVD placement.
3. Tissue Injury r/t traumatic catheter insertion evidenced by gross hematuria.
- Glasgow Coma Scale (1,2)
- Level of Conciousness (1,2)
- Level of Orientation (person, place & time) (1,2,)Ask about level of pain on a scale of 0-10, 0 being no pain at all and 10 being the worst pain possible. Ask where the pain is, describe what type of pain it is, how long the pain has continued for and anything that brought on the pain (PQRST method). Administer pain meds as neccessary. (1,2,3)
- Pupillary Reflex- assessing whether they are equal, brisk or sluggish and what size (1,2)
- Activity and Movement-check for movement of all limbs and strength of handgrips, arms, legs, plantar flexion and dorsiflexion. Rate the strength of each limb according to weak, moderate and strong and if its equal bilaterally. Take note of the patient’s activity level which in this case is bedrest. (2)
- Sensation-ask if the patient is experiencing any feelings of numbness or tingling. Identify where its locate and if the feeling radiates elsewhere. (2)
- EVD- note the amount, color and consistency of the fluid draining from the EVD. Look for any present blood clots. (2)
- Color (pallor, erythema, cyanosis, jaundice or congruent with skin type). Assess the body for skin color throughout, pay special attention to the nailbeds and lips for cyanosis which would indicate respiratory distress. (1,2)
- Temperature-take an oral temperature. Feel for skin temperature with the dorsal side of your hands over all areas of the body,comparing symmetric spots. (1,2,3)
- Perpheral Pulses- carotid, radial, brachial, popliteal, dorsalis pedis and posterior tibial pulses. Rate each pulse from 0-4 and compare bilaterally. Also check cap refill and skin turgor. (2)
- Edema- Look for any edema throughout the extremities. If any pitting edema is noted grade it from +1-4.
- Heart sounds- inspect, palpate, percuss and auscultate the heart
- Vital Signs- TPR, BP & O2 sats (1,2,3)
- SOB/SOBOE- observe/ask the patient if they feel short of breath. (1)
- Respiratory rate- assess the rhythm, rate, the position they take to breath and any use of accessory muscles.(1)
- Trach secretions-note the amount, consistency and color of the secretions. Apply suction as necessary. (1)
- Cough- is it productive or not. Observe whether the client is able to clear their own secretions. (1)
- Breath sounds-inspect, palpitation, percussion, auscultate lund fields. (1)
- O2 sats- assess if the client needs additional oxygen. (1)
- Diet- how well the patient tolerates their fully thickened fluid diet by observing them eatting. Ask them if they have an appetite. (1)
- Nausea/Vomiting- is the patient experiencing any nausea. Adminster gravol as neccessary. (1,2,3)
- Abdomen- inspect, auscultate, percuss and palpate the abdomen. Note if the abdomen appears scaphoid, distented, rounded or flat. Listen for bowel sounds in all four quadrants. (3)
- Catheter- assess the I & O ratio, color, amount and consistency of the urine. If gross hematuria continues, monitor it closesly throughout the day. (3)
- Bowel/Bladder patterns- take note of the patients last bowel movement. When changing the benefits look for incontinence of stool.
- Skin condition- observe the skin for temperature, moisture, texture, thickness, bruising, and lesions. (2,3)
- Dressings-inspect the dressing for any drainage. Lightly palpate over the dressing for any lumps. (2)
- Inspect the groining for tissue breakdown related to catheter insertion (3)
- Coping-ask the patient how he’s coping with being in the hospital, reduced verbal communication and the change to his present health status.
- Visitors-ask if he will have vistors in to see him.
- Mood/Affect- ask about the patient’s mood and monitor if it’s congruent with his affect.
Neuro Vital Signs
Nervous System Assessment
- Assessment if mental status, cranial nerves, cerebellar function, sensory & motor system and reflexes.
Neuro Vital Signs/
- Assess intracranial activity by looking at level of consciousness (LOC), vital signs, pupilary reaction, and motor responses.
- Score ranges from 3-15.
- Other considerations that could alter assessment: intubated, eyes swollen closed, paralyzed, doesn’t speak English, deaf, aphasic, blind.
- detects life-threatening complications such as cerebral edema
- How would you assess infant/toddler? (crying, playing, laughter)
a. Level of Consciousness
- first change with altered cerebral tissue perfusion
1. Response to touch-
- call patient by name before touch and ask to open eyes
- if no response, repeat stimulus in both ears, loudly
- If no response, touch patient firmly and repeat command. If no response, notify RN
2. Orientation
- Person (Please tell me you name/ what’s your name?)
- Place (What building are you in? City? Province?)
- Time (What is today’s date? Day of the week? Month? Year? Season?)
B. Pupils
- eye opening
- talk and observe response
- avoid direct light
- estimate pupil size(
- Use flashlight from periphery of eye to determine response (
- Repeat on other eye (check for bilateral/unilateral concerns)
C. Motor Response
- Increased ICP at cortical levels leads to abnormal flexion posturing. As it increase at pons, it leads to abnormal extension posturing. At medulla there is flaccidity. No response is worst.
- Upper limbs
- ask client to move limbs
- Use 2 fingers and ask client to grab them firmly.
- ask client to release grip ( grip may be reflex, release is cognitive)
2. Lower Limbs
§ ask client to move limbs
§ ask client to push against resistance ( test bilateral at same time)
D. Sensory response
1. Have client close eyes
2. Touch client on all four limbs and ask to identify touch
E. Vital Signs
1. Take pulse, resps, BP, and report changes
2. These would be late changes
3. Record all data
Cushing’s response-
- Bradycardia, systolic hypertension, wide pulse pressure and alterations in respiratory response (bradycardia, low resp rate and wide pulse pressure is Cushing’s triad)
- Due to pressure on medulla
Signs of Increased ICP
- headache
- nausea/vomiting
- seizures
- irritability
- drowsiness
- decreased activity
- increased fatigue
- memory loss
- late signs: decreased LOC, response, alterations in pupils
Coma occurs because of extensive, diffuse, bilateral cerebral hemispheric destruction, a lesion in diencephalons, destruction of brainstem down to level of pons.
Subscribe to:
Comments (Atom)